What Is the Corpus Cavernosum and How Does the P-Shot Target It?

Most discussions of erectile dysfunction focus on hormones or psychology. Yet very few address the structural tissue at the core of penile function — the corpus cavernosum. Understanding this anatomy is essential before evaluating any treatment, including the P-shot.
This article explains the anatomy of the corpus cavernosum, its role in erection physiology, and the evidence base for platelet-rich plasma (PRP) therapy delivered directly to this tissue. Written for patients seeking accurate medical information rather than marketing material, it prioritises clinical clarity throughout.
Penile Anatomy: A Clinical Overview
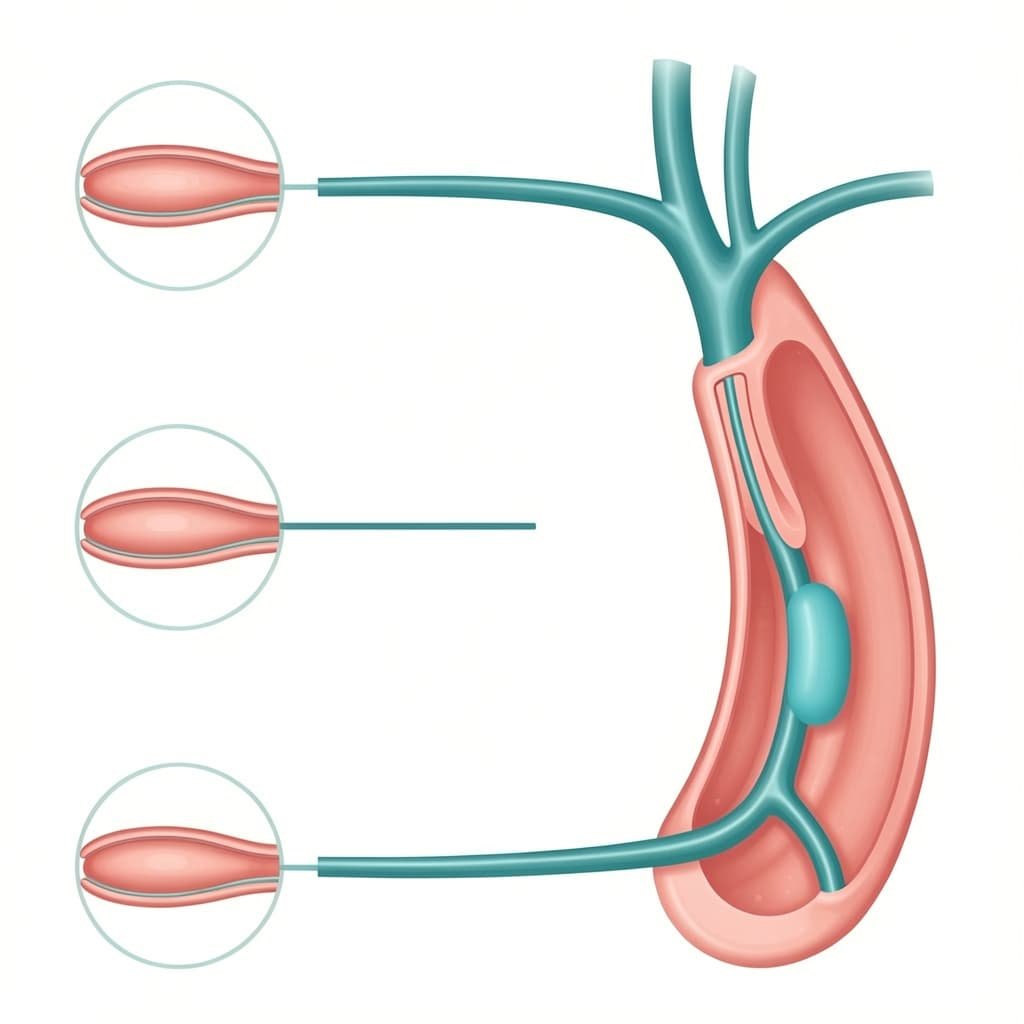
The penis contains three cylinders of erectile tissue. Two of these are the corpus cavernosa (the plural of corpus cavernosum), while the third is the corpus spongiosum, which surrounds the urethra.
Each corpus cavernosum runs along the dorsal (upper) side of the penile shaft. Together, they form the primary structural foundation of penile erection anatomy. Far from being passive tubes, these are highly vascular, innervated tissues with a complex cellular architecture.
Composition of the Corpus Cavernosum
The corpus cavernosum consists of several distinct tissue types:
• Smooth muscle cells — control blood flow by relaxing or contracting
• Collagen fibres — provide structural rigidity and elasticity
• Elastin — allows tissue to expand and return to its resting state
• Endothelial cells — line the sinusoidal spaces and regulate vascular tone
• Nerve fibres — both autonomic and somatic, controlling erection and sensation
• Sinusoidal spaces — hollow lacunae that fill with blood during erection
This cellular complexity is central to understanding why the corpus cavernosum is both vulnerable to damage and a logical target for regenerative treatment.
The Tunica Albuginea
Each corpus cavernosum sits enclosed within the tunica albuginea — a dense fibrous sheath made of collagen. During erection, this sheath compresses the emissary veins, thereby preventing venous outflow and maintaining penile rigidity. When the tunica albuginea sustains damage or scarring — as occurs in Peyronie’s disease — it directly impairs the erectile function of the corpus cavernosum.
How the Corpus Cavernosum Produces an Erection
Understanding erection anatomy requires understanding vascular mechanics. Sexual stimulation triggers the release of nitric oxide (NO) from nerve endings and endothelial cells within the corpus cavernosum.
The Vascular Sequence
Nitric oxide activates an enzyme called guanylate cyclase, which in turn produces cyclic guanosine monophosphate (cGMP). This molecule then causes smooth muscle relaxation within the corpus cavernosum, increasing arterial inflow as a result. Blood fills the sinusoidal spaces, the expanding tissue compresses the surrounding veins, and blood becomes trapped — producing a rigid erection.
Drugs such as sildenafil (Viagra) work by inhibiting the enzyme that breaks down cGMP — phosphodiesterase type 5 (PDE5). Crucially, they do not treat the underlying tissue; they amplify a signal that is already present. When endothelial cells or smooth muscle cells in the corpus cavernosum sustain damage, PDE5 inhibitors become progressively less effective.
Neural Control of the Corpus Cavernosum
The cavernous nerves, which arise from the pelvic plexus, supply the corpus cavernosum with innervation. These nerves carry parasympathetic signals that initiate smooth muscle relaxation, as well as sympathetic signals that cause detumescence (loss of erection). Any disruption to these nerves — whether surgical, diabetic, or traumatic — directly impairs corpus cavernosum function.
Erectile dysfunction (ED) following radical prostatectomy is common for precisely this reason. Because the cavernous nerves run adjacent to the prostate gland, surgical trauma to these nerves produces neurogenic ED through corpus cavernosum denervation.
Pathological Changes in the Corpus Cavernosum
The NHS recognises that erectile dysfunction affects approximately half of men aged 40 to 70 in the United Kingdom. In most cases, the underlying cause is vascular or neurogenic — and both affect the corpus cavernosum at a cellular level.
Endothelial Dysfunction
Endothelial cells lining the sinusoidal spaces of the corpus cavernosum produce nitric oxide. Chronic conditions — particularly diabetes, hypertension, and hyperlipidaemia — damage endothelial function, causing nitric oxide production to fall. Smooth muscle cells consequently become fibrotic, and the structural elasticity of the corpus cavernosum declines.
A study published in the Journal of Sexual Medicine demonstrated that penile endothelial dysfunction precedes systemic cardiovascular endothelial dysfunction in many men. As a result, NICE now recognises ED as a potential early marker of cardiovascular disease.
Smooth Muscle Fibrosis
Progressive fibrosis of the corpus cavernosum smooth muscle reduces its ability to relax. Rather than a purely functional change, this represents a structural alteration. The ratio of smooth muscle to connective tissue within the corpus cavernosum decreases with age and with conditions such as diabetes. Fibrotic tissue cannot expand to accommodate blood, so erections become incomplete or absent.
Peyronie’s Disease
Peyronie’s disease involves the formation of fibrous plaques within the tunica albuginea, directly adjacent to the corpus cavernosum. These plaques cause penile curvature, pain, and in many cases erectile dysfunction. Furthermore, the mechanical distortion of the corpus cavernosum disrupts uniform blood distribution during erection.
What Is the P-Shot and How Does It Work?
The Priapus shot — commonly referred to as the P-shot, P shot, Pshot, or priapus shot — is a non-surgical treatment for erectile dysfunction that uses platelet-rich plasma (PRP). Unlike pharmaceuticals, it does not introduce foreign substances. Instead, it uses the patient’s own blood, processed to concentrate growth factors, then injected directly into the corpus cavernosum.
Platelet-Rich Plasma: The Scientific Basis
Platelets are small cell fragments circulating in blood, primarily associated with clotting. However, platelets also contain alpha granules packed with growth factors, including:
• Platelet-derived growth factor (PDGF) — stimulates cell proliferation
• Vascular endothelial growth factor (VEGF) — promotes new blood vessel formation (angiogenesis)
• Transforming growth factor-beta (TGF-β) — regulates tissue remodelling
• Epidermal growth factor (EGF) — supports epithelial and endothelial repair
• Insulin-like growth factor (IGF) — supports smooth muscle maintenance
When concentrated PRP reaches damaged tissue, these growth factors activate local stem cells and progenitor cells. They promote new capillary formation, reduce fibrosis, and support cellular regeneration.
The P-Shot Injection Site: The Corpus Cavernosum
The corpus cavernosum itself serves as the P-shot injection site — a deliberate anatomical choice. As the primary vascular tissue of the penis, delivering PRP directly into this structure allows growth factors to act on the endothelial cells, smooth muscle cells, and nerve endings that govern erectile function.
The procedure requires precise anatomical knowledge. Under local anaesthetic, a fine needle delivers the PRP into the lateral aspect of the penile shaft, targeting the corpus cavernosum bilaterally. Both the corpus spongiosum and the urethra are avoided throughout.
This requirement for precision makes the clinician’s expertise critically important. The P-shot injection site tolerates no imprecision.
4.3 Proposed Mechanisms Within the Corpus Cavernosum
PRP therapy for men’s performance issues works through several proposed mechanisms:
• Stimulation of endothelial progenitor cells to rebuild damaged sinusoidal lining
• Promotion of new capillary growth within the corpus cavernosum via VEGF
• Reduction in smooth muscle fibrosis through anti-inflammatory growth factors
• Support of cavernous nerve regeneration following neurogenic injury
• Improvement in nitric oxide availability through restored endothelial function
These mechanisms align with the known cellular pathology of erectile dysfunction and with the established science of PRP in other regenerative medical contexts, including orthopaedics and wound care.
What Does the Evidence Show?
The evidence base for PRP-based regenerative therapy for ED continues to grow, though it remains at an early stage. The following is an honest summary of the current literature.
Clinical Studies
A randomised controlled trial by Matz et al. (2018), published in the Journal of Sexual Medicine, found that intracavernosal PRP injection produced statistically significant improvements in International Index of Erectile Function (IIEF) scores compared to placebo. Participants reported improvements in both erection quality and sexual satisfaction.
A 2021 systematic review by Poulios et al. examined PRP therapy for erectile dysfunction and concluded that intracavernosal PRP — directly targeting the corpus cavernosum — was associated with measurable improvements in erectile function. Nevertheless, the authors noted that larger randomised controlled trials are needed before definitive clinical guidelines can be issued.
A study published in Andrologia (2020) assessed advanced PRP solution for erectile dysfunction in men with mild to moderate vasculogenic ED. Patients showed improvement in IIEF scores at both three and six months, and no serious adverse events were reported throughout.
Evidence in Peyronie’s Disease
Several studies have examined intracavernosal PRP in men with Peyronie’s disease. A 2019 prospective study found reductions in plaque size and penile curvature following serial PRP injections. Participants also reported improvements in erectile function, and in all studies reviewed, the corpus cavernosum served as the primary target tissue.
Limitations of the Current Evidence
Both clinicians and patients must acknowledge significant limitations in the current evidence:
• Most studies have small sample sizes
• No standardised PRP preparation protocol yet exists
• Platelet concentrations and activation methods vary between studies
• Long-term outcome data beyond 12 months remain scarce
• Placebo-controlled trials are methodologically challenging in procedural medicine
The British Society for Sexual Medicine (BSSM) does not yet include PRP as a first-line recommendation for erectile dysfunction treatment. However, the society acknowledges the emerging evidence base and does not contraindicate its use in appropriately selected patients.
Who May Be Suitable for the P-Shot?
The P-shot is not appropriate for all men with erectile dysfunction. Patient selection is central to achieving realistic outcomes, and the following profiles are commonly considered in clinical practice.
Vasculogenic Erectile Dysfunction
Men with vasculogenic ED — where impaired blood flow stems from endothelial dysfunction — represent the population most likely to benefit from regenerative treatment for male health in the UK. In this context, the corpus cavernosum endothelium serves as the primary target of PRP.
Peyronie’s Disease
Men with Peyronie’s disease, where fibrous plaques affect the tunica albuginea adjacent to the corpus cavernosum, have featured in multiple small clinical trials. Evidence suggests PRP may reduce inflammation and fibrous deposition in early-stage disease.
Post-Surgical or Post-Radiotherapy ED
Men who have undergone radical prostatectomy or pelvic radiotherapy often develop neurogenic or vasculogenic ED. Although PRP-based regenerative therapy has shown promise in supporting nerve recovery in early post-surgical animal models, human data remain limited at present.
Men Seeking Non-Surgical Treatment
Some men prefer a natural ED treatment using PRP therapy over pharmaceutical options. For those who experience side effects from PDE5 inhibitors — such as headache, flushing, or visual disturbance — or for whom these drugs are contraindicated due to cardiac conditions, the P-shot offers an alternative non-surgical approach to erectile dysfunction care in London and across the UK.
Men Considering Penile Injection Growth
Some patients enquire about the P-shot in the context of penile injection growth or penile enlargement. To date, evidence for dimensional change following PRP injection remains limited. One small study reported modest increases in penile length and girth in participants who also used vacuum erection devices alongside PRP, though these findings require larger replication studies before conclusions can be drawn.
P-Shot Before and After: What Patients Report
Published P-shot before and after data — drawn from both clinical studies and patient-reported outcomes — describe the following changes:
• Improved erection firmness in men with mild to moderate vasculogenic ED
• Increased sensitivity in the glans and shaft
• Improved response to PDE5 inhibitors in men where pharmaceutical therapy had plateaued
• Reduced penile curvature in early Peyronie’s disease
• Improved self-reported sexual confidence and satisfaction
In clinical literature, P-shot before and after comparisons typically use the IIEF-5 questionnaire for measurement. This validated five-item tool assesses erectile function, intercourse satisfaction, orgasmic function, sexual desire, and overall satisfaction.
Results vary between individuals. Factors that influence outcome include the severity of pre-existing endothelial damage, age, comorbidities, and the PRP preparation technique applied. It is therefore inaccurate to present the P-shot as a universal cure for erectile dysfunction.
8. The Procedure: What Happens During a P-Shot Treatment
Men’s intimate health treatment in London — when a qualified clinician performs it — follows a structured protocol. Standard clinical practice proceeds as follows:
• A small volume of blood is drawn from the patient’s arm — typically 30 to 60 ml
• Centrifugation separates platelet-rich plasma from red blood cells and platelet-poor plasma
• The PRP undergoes activation — either with calcium chloride or left unactivated depending on the protocol
• A topical anaesthetic cream is applied to the penis for 20 to 30 minutes
• A local anaesthetic nerve block is administered at the base of the penile shaft
• The PRP is injected directly into the corpus cavernosum — bilaterally in most protocols
• In total, the procedure takes approximately 45 to 60 minutes
The corpus cavernosum is accessed via the lateral shaft at a defined anatomical point, carefully avoiding the dorsal nerve, urethra, and corpus spongiosum. Following the procedure, clinicians often recommend a vacuum erection device to encourage PRP dispersion and maintain penile blood flow during recovery.
Safety, Side Effects, and Contraindications
PRP is an autologous treatment — meaning it uses the patient’s own blood. This approach eliminates the risk of allergic reaction or disease transmission from external sources, and the published literature reports a consistently low adverse event profile.
Common Side Effects
• Temporary bruising or swelling at the injection site
• Mild discomfort lasting 24 to 48 hours
• Temporary hypersensitivity in the treated area
Rare Complications
• Haematoma (blood pooling) within the corpus cavernosum
• Infection (rare given the sterile technique required)
• Priapism — prolonged, unwanted erection — theoretically possible but rarely reported
Contraindications
• Active genital infection or skin condition
• Platelet dysfunction disorders or thrombocytopaenia
• Anticoagulant therapy (relative contraindication — requires clinical assessment)
• Active cancer — particularly haematological malignancy
• Severe arterial insufficiency requiring surgical intervention
A thorough medical history, examination, and appropriate investigations — including penile Doppler ultrasound in selected cases — should precede any P-shot treatment decision.
Cost and Access in the UK
Priapus shot pricing in the UK varies between clinics. In London, costs typically reflect the clinic’s facilities, the clinician’s credentials, and the PRP preparation system in use. Generally, P-shot UK pricing ranges from approximately £800 to £2,000 per session across most private London clinics.
The treatment does not appear on the NHS and classifies as a private, elective procedure. Before proceeding, patients should verify the qualifications of the clinician, the sterility of the preparation environment, and the PRP system employed.
Priapus shot London services are available at a number of Harley Street and Marylebone-based private practices. Dr Syed Nadeem Abbas at pshots clinic uk offers this treatment within a regulated private medical environment, with full clinical assessment preceding any intervention.
Frequently Asked Questions
What exactly is the corpus cavernosum?
The corpus cavernosum is one of two paired cylinders of erectile tissue within the penile shaft. Each one contains smooth muscle, collagen, elastin, and vascular sinusoidal spaces that fill with blood during erection. Understanding the corpus cavernosum is therefore central to understanding both erectile function and dysfunction.
Why is the P-shot injected into the corpus cavernosum specifically?
Because the corpus cavernosum is the primary vascular tissue governing erection, delivering PRP directly to this structure allows growth factors to act on the endothelial cells and smooth muscle cells most affected by vasculogenic or fibrotic ED. Peripheral injection would not achieve the same cellular contact.
How many P-shot sessions are typically required?
Most clinical protocols involve one to three sessions, spaced four to six weeks apart. Some patients report benefit after a single session, while others require serial treatment for sustained improvement. Depending on individual response, clinicians may also recommend annual maintenance injections.
Is the P-shot painful?
Although injection into the penis sounds uncomfortable, topical and local anaesthetic applied before the procedure effectively numbs the area. In practice, most patients report minimal discomfort during treatment itself. Some post-procedure sensitivity is normal for 24 to 48 hours.
Does the P-shot work for all types of erectile dysfunction?
No. Evidence most strongly supports the P-shot for vasculogenic and early neurogenic ED. It is not a replacement for testosterone therapy in men with hypogonadism, nor suitable for severe arterial disease requiring surgical revascularisation. A thorough clinical assessment must precede any treatment decision.
Can the P-shot be combined with other ED treatments?
Yes. PRP therapy is frequently combined with PDE5 inhibitors, low-intensity shockwave therapy (Li-ESWT), or vacuum erection devices. Indeed, some evidence suggests that combination approaches — particularly PRP with Li-ESWT — produce better outcomes than either treatment alone, making this an active area of ongoing clinical research.
What is the difference between the P-shot and penile fillers?
The P-shot delivers platelet-rich plasma to the corpus cavernosum for regenerative purposes, whereas penile fillers use hyaluronic acid injected into the subcutaneous layer of the shaft or glans for girth enhancement. Targeting different anatomical layers and serving different clinical purposes, these are not interchangeable treatments.
How long does the P-shot last?
Duration of effect varies between individuals. Most published studies report outcome data at three to twelve months, with some patients reporting sustained benefit beyond the 12-month mark. Cellular regeneration is not a permanent process, however, and the underlying condition causing ED does not disappear. Lifestyle factors, cardiovascular health, and diabetes control all influence long-term outcomes.

Conclusion
The corpus cavernosum is not simply a passive structure. Rather, it is a dynamic, vascular, innervated tissue that sits at the centre of male erectile physiology. Its cellular architecture — endothelial cells, smooth muscle, collagen, sinusoidal spaces — is vulnerable to damage from ageing, vascular disease, diabetes, surgical trauma, and fibrosis.
The P-shot, or Priapus shot, targets the corpus cavernosum directly, delivering autologous platelet-rich plasma to the specific tissue layer where erectile dysfunction most commonly originates. Although the evidence base supporting PRP-based regenerative therapy for ED continues to grow, it is not yet sufficient to establish first-line clinical guidance.
Patients considering this treatment must therefore engage in an honest clinical conversation. The P-shot is not a guaranteed cure; outcomes depend on the underlying pathology, the PRP preparation method, the clinician’s anatomical precision, and broader patient health factors. It is, however, a promising, evidence-informed option within a wider approach to men’s intimate health — not a replacement for comprehensive assessment and management.
Informed decision-making in erectile health requires understanding both the anatomy involved and the evidence available. The corpus cavernosum is where erection begins — and where evidence-based regenerative treatment must, logically, also begin.
If the primary structural tissue of erection can be regenerated rather than merely stimulated — what does that mean for how we should approach erectile dysfunction care in the decade ahead?
Read more: Talking to Your Partner About the P Shot – A Practical Guide
Does Private Insurance Cover the P Shot UK? What Patients Need to Know